New paper: TDCS for gait-therapy post-stroke
Pundik S, Skelly M, Salameh A, Leonhardt L, Hardin EC, Hisel T, Duncan KR, Zink E, Carr SJ, Mosca L, Yaghmoor B, Bikson M, Daly JJ, McCabe J. Transcranial direct current stimulation with motor-learning based gait therapy post-stroke: A randomized controlled trial. Brain Stimul. 2026 May 29;19(4):103132. doi: 10.1016/j.brs.2026.103132. Epub ahead of print. PMID: 42217542.
Abstract
Background: Persistent gait deficits after stroke are prevalent and negatively impact function. Motor learning methods promote neuroplasticity and can produce significant clinical gains, however recovery is limited for many individuals in the chronic phase. Transcranial direct current stimulation(tDCS) can enhance neuroplastic effects of training and can be easily paired with neurorehabilitation.
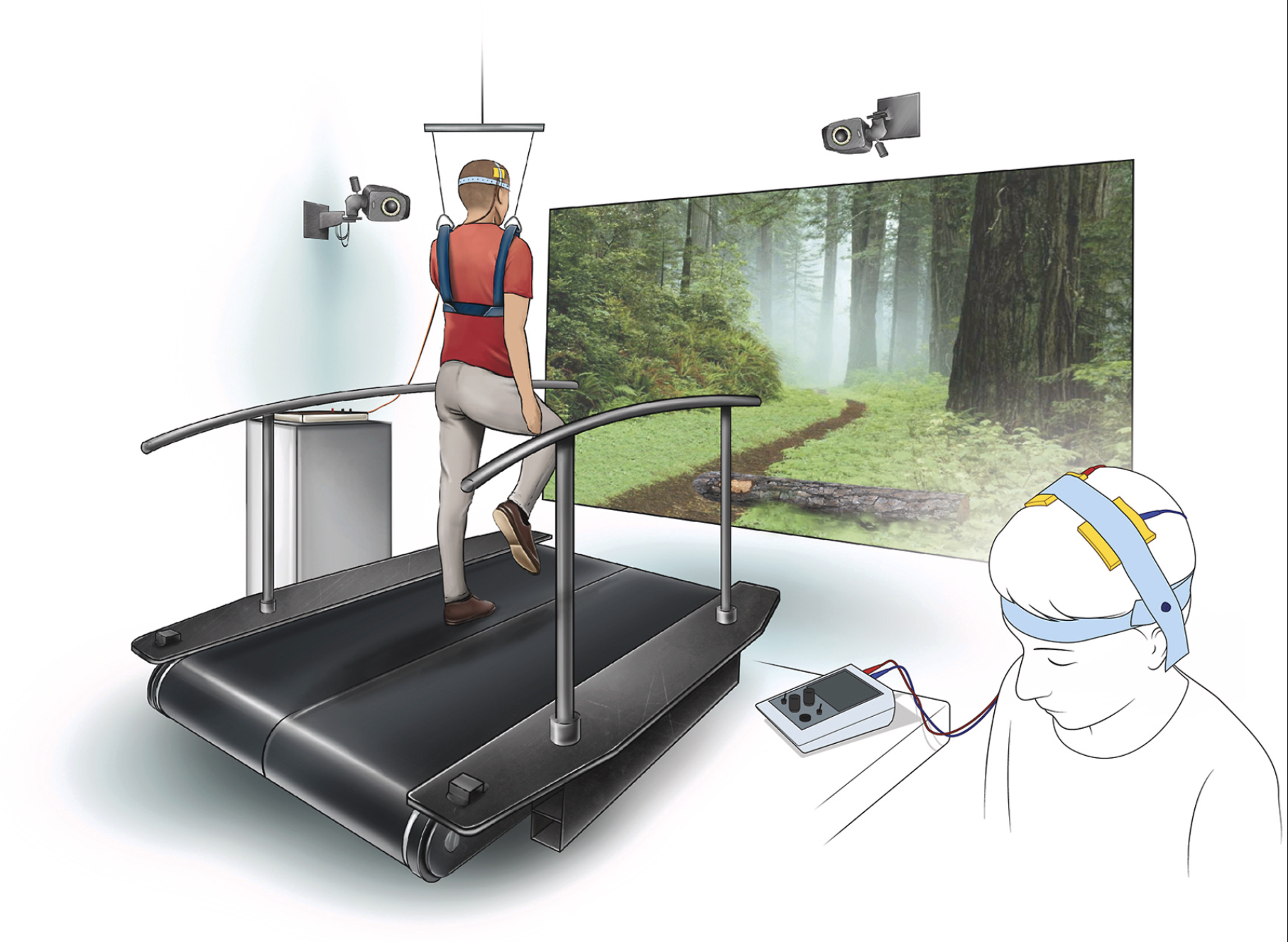
Objective: We tested active vs. sham bihemispheric 2 mA tDCS targeting primary motor leg regions paired with gait therapy.
Methods: Individuals(n = 44) were randomized to 10 sessions of active tDCS/sham tDCS paired with motor training. Outcomes were collected at baseline, mid-treatment, post-treatment and 6-week follow-up. TDCS-induced electric field(e-field) and lesion load were calculated using each participant's magnetic resonance imaging (MRI). Statistical methods included longitudinal linear mixed-effects model with treatment group by time interaction effects, Wilcoxon signed rank test and correlation analyses.
Results: Thirty-nine individuals completed the study. No difference was observed between treatment groups. Total cohort analysis showed significant improvement (p < 0.05) in the following: Fugl-Meyer, fastest gait speed, preferred gait speed, Timed Up and Go, Functional Gait Assessment, and Gait Assessment and Intervention Tool across time, with maintenance or improvement at 6-week follow-up. E-field in targeted region ranged 0.10-0.29 V/m. Lesion load did not correlate with change in clinical outcomes.
Conclusions: Both groups improved across the clinical outcomes following short duration motor learning-based gait training with and without tDCS. Lesion load was not related to treatment response. E-field in targeted regions was variable across participants. Future studies employing optimized tDCS to ensure consistent dosing across subjects, paired with an effective gait training approach is needed.
Keywords: Brain stimulation; Electric field modeling; Gait; Lesion load; Motor learning; Rehabilitation; Stroke; Transcranial direct current stimulation; Virtual reality.